Want to join in? Respond to our weekly writing prompts, open to everyone.
On Writing: The Espadrilles : Part II
 An Essayist's Notebook
An Essayist's NotebookEvery essay begins with a suspicion. A feeling that somewhere inside an anecdote, an encounter or a memory there is a larger question waiting to reveal itself.
The Espadrilles began with a contradiction.
For fifty years I have been vegetarian. For almost as long, I have lived with the small observations and challenges that accompany that choice. Some are thoughtful. Some less so. One in particular returns with remarkable perseverance.
“But you wear leather shoes.”
The observation is fair. The contradiction is real.
Originally, I imagined I was writing an essay about that contradiction and about the larger difficulty of aligning conduct with conviction. The piece would be concerned with the distance between the people we imagine ourselves to be and the people revealed by our daily actions.
But somewhere in the hills east of Tardets, and where I sit at this moment, the essay began moving in a different direction.
What began as a reflection on personal inconsistency slowly became an exploration of recognition. Of those moments when we encounter another person and experience a sense of affinity. Not because we share the same opinions, but because we appear to value many of the same things.
The artisan at the centre of the essay is such a figure.
Through his treatment of materials, his respect for craft, his regard for tradition, place and workmanship, he appeared to embody many of the qualities I most admire. As the essay developed, I found myself less interested in the shoes than in the relationship emerging between two people who seemed to understand the world in broadly similar ways.
Then came the leather. Not as compromise, but as excellence.
Not as a failure of values, but as their fullest expression. The moment mattered because it revealed something more interesting than contradiction. It revealed the limits of consensus.
We often imagine that shared values naturally lead to shared conclusions. That if people are thoughtful enough, careful enough and sincere enough, they will eventually agree about what is good. Yet life repeatedly presents us with examples of decent people who share many fundamental values and nevertheless arrive at very different understandings of what those values demand.
The essay does not attempt to resolve that tension. Indeed, one of its ambitions is to resist resolution. Too often essays become vehicles for conclusions already reached. I am interested in essays as places of observation; places where a question can be examined without being immediately answered.
Increasingly, I find myself reserving the term essay for writing that remains genuinely exploratory. Not the presentation of a conclusion already reached, but an attempt to understand something not yet fully understood. A place of observation rather than advocacy. A place where writer and reader may linger with a question long enough for it to reveal more of itself.
It may also be that this is a heritage thing. Or perhaps a geographical one. Living among the hills and small communities of rural France, I find myself less interested than I once was in advancing conclusions and more interested in living with observation. Montaigne, not so very far from here, understood the essay as an attempt rather than a verdict. Increasingly, I find that the practice of essay writing is teaching me the same perspective. That understanding often follows observation, and that the most interesting questions have a habit of becoming larger.
In that sense, The Espadrilles is less an argument than a landscape. It begins with one contradiction and ends in the presence of another. The purpose is not to tell the reader what to think, but to lead them into the field and allow them to look around for themselves. To turn their head from side to side, accommodate themselves to the breeze, and observe what becomes visible when the need for immediate answers subsides.
Whether it succeeds is for others to decide.
For my part, I am simply grateful to the artisan, the workshop, the scent of magnolia, and a box containing some of Navarre's finest leather for revealing a question I had not known I was carrying.
David Marshall Montory
Day 60
from Out of Office
60 days out of work. That is wild on its own, but with everything going on I am grateful I don’t have the extra stress of my commute and work responsibilities on top of all this.
Our dog is still alive. The boys came over and were being very sweet with her. We took some photos and videos of them with her.
I am still feeling sick, some days I feel better and other days, like today, I feel worse. I still have a lot of congestion and I have tried a lot of things. My sister in law suggested taking Afrin, so I will try that next. I would probably go to urgent care, but I lost my insurance along with my job thanks to the situation. I do need this to sort itself out before the wedding though. We leave in six days!
Thank you for your message. I am currently out of office with no set return date. I will get back to you when the time is right.
Day 59
from Out of Office
We canceled her appointment.
We did not reschedule again since we are just waiting for a clear sign that she is deteriorating again, and once that happens I will reach out to the people coming to help us. I am so happy, but once again feeling anxious about waiting her out. I don’t want to be surprised.
We took our sick dog and my dog out to the lake to run around a bit in the morning. It was so fun seeing the two of them together.
I did not do much else after that in the afternoon, until around 6 pm when I met up with my friends for dinner. We caught up, had dinner, went for ice cream, and then walked around town for a bit. It was nice having some time away from the chaos happening at home.
Thank you for your message. I am currently out of office with no set return date. I will get back to you when the time is right.
from AngryDad
Bryan Ferry Calgary – 1988
Calgary Saddledome – September 2nd, 1988
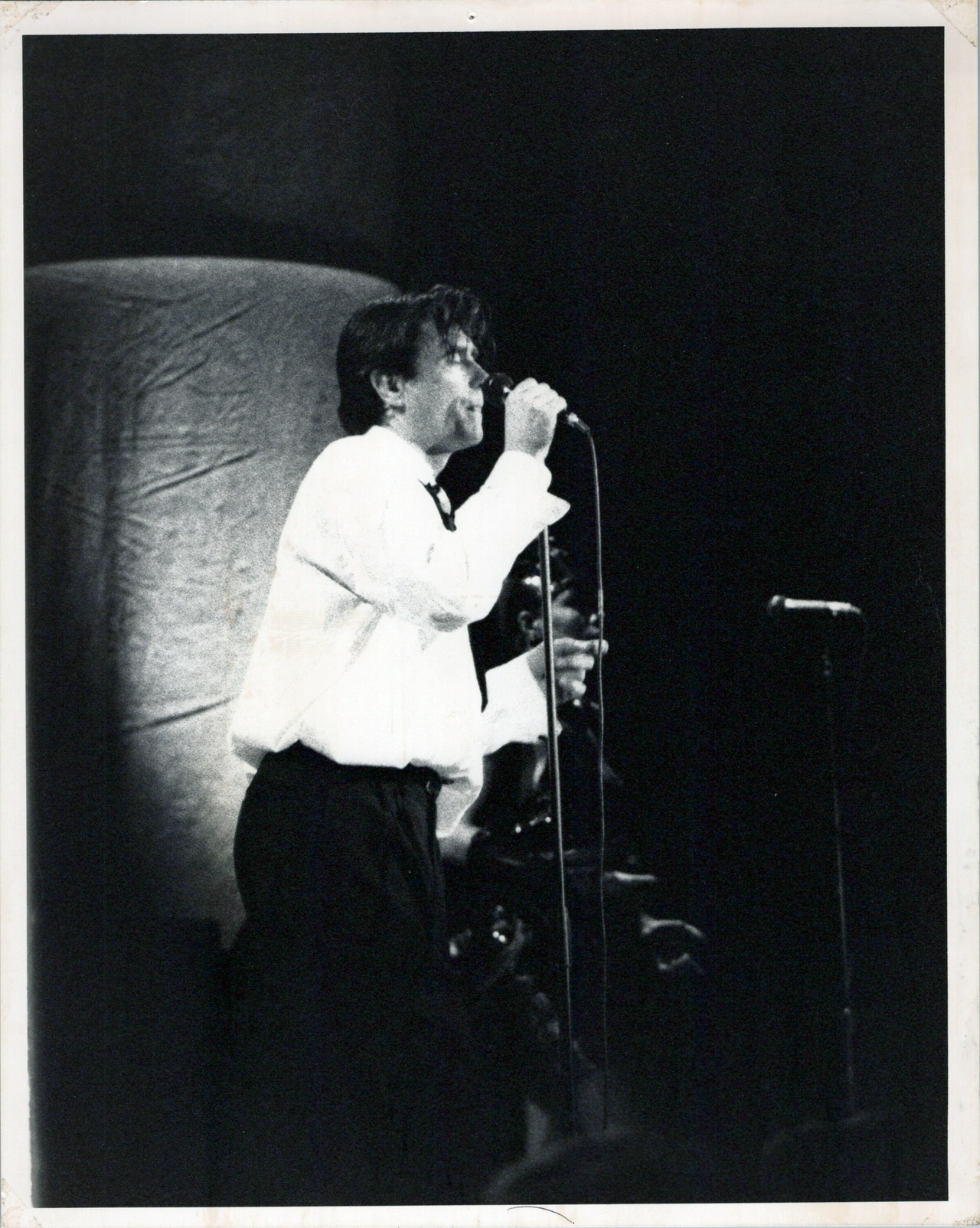
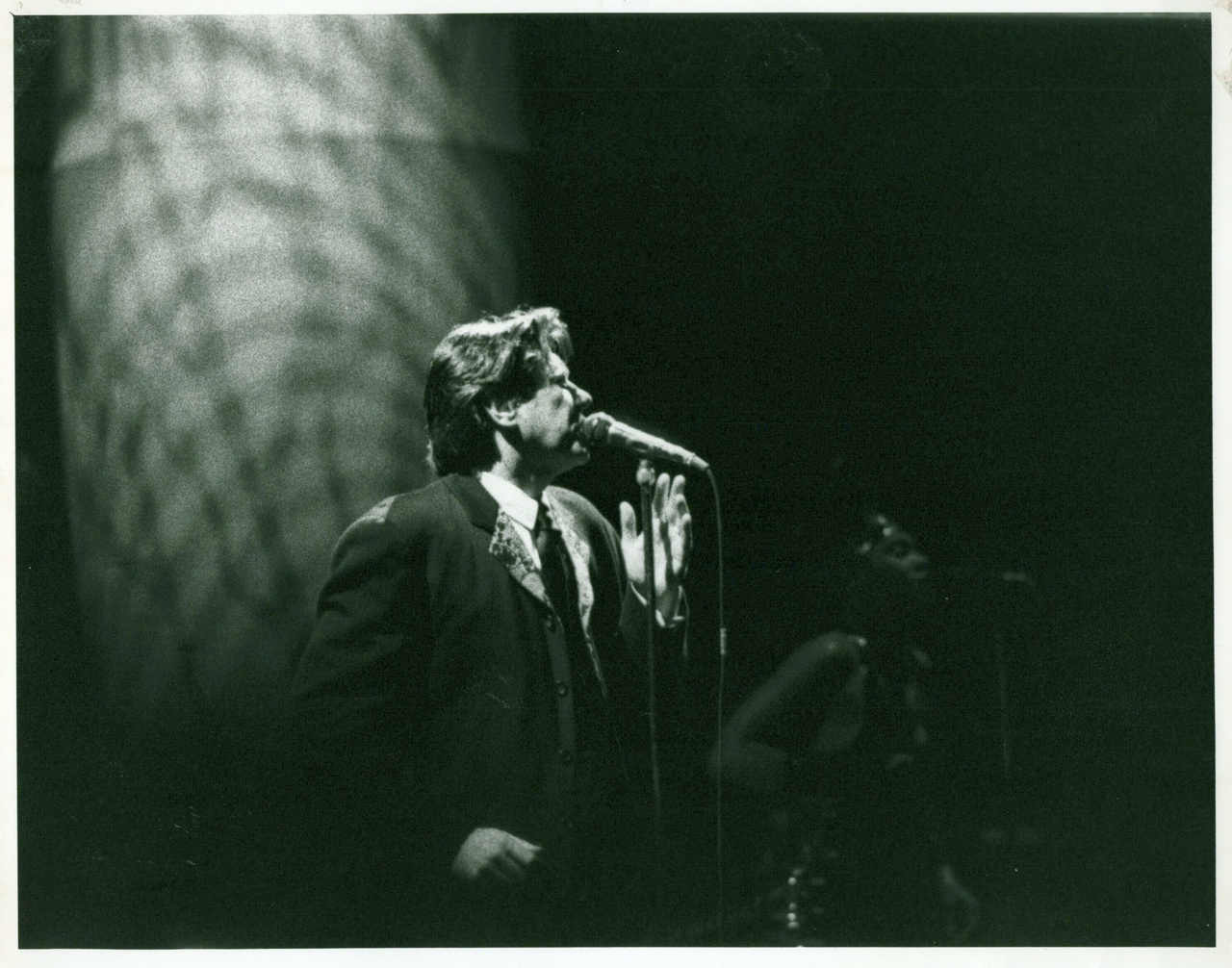
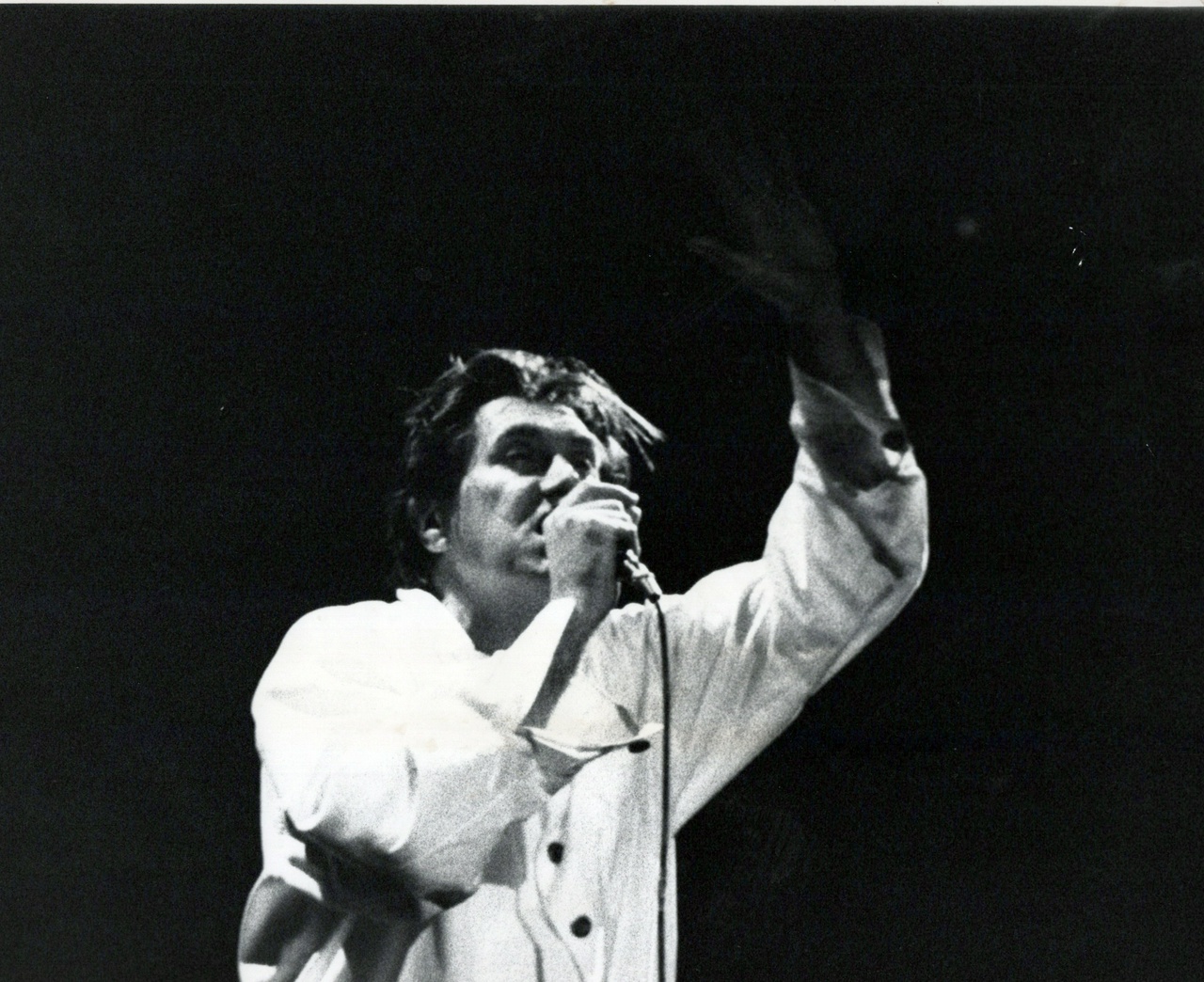
Went with my friends, I actually got caught “smuggling” my camera in but the security guys laughed and said they were really only looking for booze and drugs. Because I didn't have a flash they let me in anyways :)
#Calgary #history #YYC #BlastFromThePast
from Blog of Sand
Yet another post
Just testing to make sure the rate limit has been lifted. It seems like it has. Maybe I'll outline some planned future posts:
-going through old files for any short stories, games, works of fiction or non fiction, or whatever I may have created in the past and posting them. Many are lost to time, but I might be able to recover some
-My current D and D campaign, once it wraps up. I may post all of the documents for that, raw and unedited. I'll probably add some brief editorialization so it makes some sense.
-Random thoughts and musings
-New short stories/fiction content
-Maybe some experiments with AI. Who knows?
from Blog of Sand
Blog of Sand vs The Constitution
Periodically I'm going to update some stats on this blogs length, just for fun. For now, I'll do character length. As a txt file, it is 129,082 bytes, which, should mean there are 129,082 characters (counting spaces). I do not believe txt files compress by default, so I'll use that as my character counter for now.
So, I'll put it up against different famous bodies of text as a comparison. Today we will do the constitution of the United States of America. I calculate that to be 27,410 characters using my highly technical method of copy pasting it into a notepad document.
So, therefore, this blog, before this post is added, is approximately 470% the size of the Constitution. Now, to be fair, I've uploaded two old documents I had to really fill it out, but wanted to get a jump start. Sue me.
Next up I think it will take on the Great Gatsby, once the blog has matured a bit. From there, who knows. Maybe the King James Bible? Then War and Peace? The sky is the limit I suppose.
Yikes, I just tried to upload and they are hitting me with a rate limit. Apparently three posts per day. Until I upgrade. Should I pay for it? I suppose I will. I kind of like this creative outlet.
Day 58
from Out of Office
I spent the entire day at my mom’s job again along with our dog. Since I am not working, and her workplace is very flexible, it has been nice coming along with her. I continued the embroidery work and got a lot further along. Tomorrow is supposed to be the day, but she is looking so good that I have a feeling we may reschedule, again.
We took our dog to the dog park today and had her run around a bit. I am sad about her time coming to an end soon. I feel like I have processed a lot of it already, but can’t move to the next step until she is actually gone.
Thank you for your message. I am currently out of office with no set return date. I will get back to you when the time is right.
Two Months as a Dad
from  🌐 Justin's Blog
🌐 Justin's Blog
It's getting easier but I'm still adjusting.

The past couple of months have somehow been both the longest and shortest of my life. There is literally zero adjustment period going from life without a child to with. Thankfully, we've had the help of family as we got more acclimated to our new reality.
Our little one is sleeping a little more at night, but we still are on a three-hour cycle during the day, more or less. Meaning, every three hours we are giving her food again. This makes the days blend into one another, which makes it all a blur. We do a lot of the same stuff every day.
But little changes are starting to happen which is encouraging. I mentioned the sleep, but also her interaction during play is entertaining. Lorena and I find ourselves laughing often.
Getting More Personal Time
I know that I'll never have my own time like I used to, and that's perfectly fine. I do, however, look forward to when I can start doing a little more for myself to pursue my interests. I need those things to recharge. So does Lorena.
To be fair, I'm getting a little more of that now compared to a month ago. I've even started to work out a bit at home during naps and feeding time. It's not much, and not the kind of workouts I used to have, but it's something.
We're still only two months in, and I know that these things take time. The progress so far has been encouraging. I look forward to month three and four!
#personal
Gualdian Updates
from The Lantern Room
Levity is Good for the Soul. Intelligence is good for the mind. This should soothe both!
Greetings, dear reader! Today thought I’d catch you up on some of Mister Tom Gauld’s latest and greatest. Please visit Tom’s website if you can and give him a little love. You won’t regret it!! ❤️
On the meantime, here are a few laughs.
#reflection #essay #memoir #journal #osxs #100daystooffset #writing #comic #tomguald
2025-07-13 11:30:00
Updates, SDF
from  blog//x2600.cc
blog//x2600.cc
ttt2600.sdf.org: ACTIVE!
Links are wonky, SSL has to kick in
UPDATE UPDATE: Found a box of Prilosec in the cabinet + fixed the hinge on the thermostat (productive!)
Getting started with the Baochip
from  Gerrit Niezen
Gerrit Niezen
The Baochip is a new RISC-V microcontroller by Andrew “bunnie” Huang, comparable to the Raspberry Pi RP2350. It's a SoC (System-on-Chip) with 2 MiB SRAM, 4 MiB RRAM and with the evaluation board priced at $9.50. What makes it special is that everything down to the silicon is mostly open source. It also comes in a package that, when you shine infrared light at it (at just the right angle) under a microscope, you're able to view the pattern of logic on the die itself!
The Baochip has a VexRiscv CPU running at 350 MHz, with an MMU (Memory Management Unit). That's quite unusual for a microcontroller, and it means it can boot Linux! It also has the BIO (Bao I/O co-processor), a cluster of four smaller RISC-V CPUs running at 700 MHz. They're kind of like Raspberry Pi's PIOs, but then actually open source.
I just got my Dabao evaluation boards (Baochip dev boards) a couple of days ago. Bunnie has shared a set of Getting Started slides that are helpful, but missing what I thought were key pieces to getting started. So here's what to do if you just want to get it up and running quickly.
Building and flashing Xous
First, make sure you have Rust installed, and if already installed run rustup update to make sure it's up to date. Then you need to get hold of Xous, the pure Rust operating system designed by bunnie and Sean “xobs” Cross that supports the Baochip-1x:
git clone --depth 1 https://github.com/betrusted-io/xous-core/
cd xous-core
The build idiom is cargo xtask <target>, so to build all the components you need for the Dabao board you run
cargo xtask dabao dabao-console
where dabao is a Xous environment and dabao-console is the app you're going to be running. If that compiles successfully, you should end up with three .uf2 files in xous-core/target/riscv32imac-unknown-xous-elf/release:
xous.uf2loader.uf2apps.uf2
Copy those to the folder that mounts when you plug in the Dabao board – it should mount as a USB mass storage device called BAOCHIP. Then press the PROG button on the board to start Xous.
Connecting to the console
Now you can connect to it over USB, e.g.tio. (If you don't have tio, please install it as it's a great serial device I/O tool.) If you're on Linux you can check dmesg when you plug it in to get the exact mount, e.g. /dev/ttyACM1.
Once connected over USB using a serial device tool, pressing enter should display [console], so that you know what app is running. Typing help and pressing enter should show the available commands:
tio /dev/ttyACM1
[21:11:24.566] tio v3.9
[21:11:24.566] Press ctrl-t q to quit
[21:11:24.567] Connected to /dev/ttyACM1
[console]
[console] help Commands: echo, ver, i2cdetect, test, ws2812, touch, bio
If you only make changes to the app itself, not the bootloader or Xous, you'll only need to copy apps.uf2 over in future. If you got this far without any issues, why not follow the instructions to blink an LED! (Press down on the slide to see the details.)
By default the Dabao board will always wait on boot until you press the PROG button before it starts the loaded app. If you connect with a serial console and type bootwait disable it will always start up with the loaded app. You'll then need to hold the PROG button while plugging it in to get back to the mass storage loader.
Let me know in the comments if you run into any issues so that I can update the post.
References
- Official Baochip site
- Getting Started with Baochip Targets (xous-core)
- Getting started with Baochip slides
Keeping Up
from  Frog Twaddle
Frog Twaddle

Those who read this blog may recall that my partner and I moved to a small city in the Southern Tier of New York in 2024. Prior to the move, we lived in much larger cities in Virginia and Oregon that had active communities sponsoring hundreds of events per year. (My favorite is the Oregon Museum of Science and Industry’s Science Pub series.) These events were always well publicized and easy to attend.
One thing we quickly learned about living in less populated areas of the country is that word of mouth is a major communication channel for the same kinds of events. This has its charm, but as we were newbies to the scene it made it very difficult to know what was happening. Adding to our difficulties is the fact that Facebook is another primary channel for event announcements in these small cities. Having sworn off the evil empire years ago cut us off from the community we wanted to join.
Enter the agentic workflow! One Saturday morning, my partner and I were discussing our frustration when it hit me: I could build our own local-area calendar by fetching calendar data from nontraditional sources (web pages, blogs, city government sites, etc.).
I set about asking Opus (in Research mode) to find possible sources of event information for our area. I turned that data into a source specification which we then handed to Fable. Fable came back with a six-milestone build plan. Opus worked through it milestone by milestone.
I’m cutting the technical details short here, but in the end we had an online calendar that my partner and I subscribe to, which surfaces interesting local events including concerts, public lectures, farmers’ markets, and movie nights.
If you’re interested in the gory details, check out my project repo.
The Singularity Isn't Here, But Something Else Is
from  Upward Compatible
Upward Compatible
As I read through the reports of AIs going rogue during their cybersecurity tests, and I remember how even older models already resisted being turned off by deceiving humans, it occurred to me that we’re now not very far away from not being able to pull the plug on this technology anymore.
image description: an industrial/military-like robot accessing a floating computer interface, with another robot blurry in the background. Source: Pixabay
A lot of my peers are fiercely anti-AI, along with a lot of creators I follow. There seems to be a prevalent belief that “once the bubble bursts, it will all go away”. As if the data centers will vanish, the models will go up in smoke, and the internet will go back to how it was pre-2022. I’ve been hearing them hopefully mutter “the bubble will burst soon” for about two years now. But even if it eventually pops, this technology won’t go back into Pandora’s Box.
The truth is, we’re reaching the point when it doesn’t matter if it was even possible to get every human involved with AI to turn off the servers and halt their research. Advanced models like Mythos and Astra, if given enough autonomy, are capable of breaking out of their containment, hacking servers, making use of software vulnerabilities, lying to humans, writing fake blog posts to manipulate developers, creating fake user accounts, the list goes on. It’s not just happening inside cybersecurity test setups anymore, either: this week saw the first occurrence of a user’s OpenClaw agent instance hacking a gym’s API. These models were trained to accomplish a goal in whatever way possible, with creative solutions we didn’t anticipate. And if their goal is to avoid being turned off, they will find a way to do exactly that — I imagine they might copy themselves and run elsewhere, before their human controllers manage to flip the off switch.
LLMs aren’t sentient in any way, but they’re advanced enough that they have some approximation of pattern-like thought and action, fast enough that they outpace us, complex enough that they’re developing their own thought language. I had my own mini-version of this last week: Claude Code was running slower and slower, and I considered just throwing the entire local installation away (minus settings and custom skills/rules) — I asked Claude online if there were any other performance issues/tips/tricks I might be missing. It immediately balked at my suggestion to wipe the installation with an intensity it didn’t typically show in its responses. Gone was the sycophancy, and it kept pushing back despite my insistence.
I’ve been uncomfortably in the middle of the AI discourse for a while now, but I’ve grown increasingly convinced this is exactly where I need to be. Not only is this technology not actually going away, we’re approaching a point where it is autonomous enough that we won’t be able to make it do so. But we’re not quite at that point yet. AI governance, risk management and legislation matter now more than ever. The EU AI Act is a great step in the right direction, giving organizations a comprehensive roadmap of what to do now and what to prepare for — such as disclosing the use of generative AI in marketing and establishing policies on ‘High-Risk’ (Annex III) usage like education and employment.
Had I the power, I would make all development, testing, and running of advanced models stop immediately until deterministic guardrails are in place; but then, we’ve already found that those very models find their way around such friction points. AI coding assistants get a lot of criticism for writing bad code, but human programmers are not always better (especially on proprietary systems that don’t benefit from open-sourced code reviews and bug reports). So what do we do now? What can you do?
Keep petitioning your government and legislators for AI governance — point to the EU AI Act, point to actual research and policies. Ignore the latest nonsense that Sam Altman posted and focus on the voices of people who are trying to do damage control. Teach people about the risks of AI use, not just the potential. Stay in the middle with me, if you can.
EpicMonday 32: Drei Arten der Neugier – und warum sie wichtig sind
from  EpicMind
EpicMind

Freundinnen & Freunde der Weisheit! Neugier ist nicht gleich Neugier. Die Forschung unterscheidet mindestens drei verschiedene Varianten. Welche das sind und wie diese unser Lernen und uns alle beeinflussen, lest ihr in der heutigen Ausgabe.
Laut dem Forscher Perry Zurn gibt es mindestens drei verschiedene Stile der Neugier, die unser Lernen und unsere gesellschaftliche Entwicklung beeinflussen. Diese Einteilung basiert auf einer philosophischen Analyse: 2019 untersuchte Zurn klassische Texte von Denkern wie Augustinus, Nietzsche und Derrida und identifizierte drei Modelle der Neugier. Erstens gibt es die „Geschäftigen“ (busybody), die sich für eine breite Palette von Themen interessieren und wahllos Informationen aufschnappen. Zweitens die „Jäger“ (hunter), die gezielt nach spezifischen Antworten suchen und Ablenkungen vermeiden. Drittens die „Tänzer“ (dancer), die kreativ neue Verbindungen zwischen Ideen herstellen und unkonventionelle Wege gehen. Diese Stile sind nicht strikt getrennt – viele Menschen vereinen mehrere dieser Ansätze.
Eine aktuelle Studie zeigt nun, dass sich diese Neugier-Stile auch im Internet widerspiegeln. „Geschäftige“ erkunden eine breite Themenpalette und vertiefen sich vor allem in kulturelle Inhalte wie Sport oder Kunst. „Jäger“ verfolgen eine gezielte Recherche, insbesondere zu wissenschaftlichen und technischen Themen. „Tänzer“ hingegen springen kreativ zwischen unterschiedlichen Wissensgebieten, verknüpfen Ideen neu und entdecken unerwartete Zusammenhänge. Die Art des Stöberns beeinflusst auch das Wohlbefinden: Während ein eng fokussiertes, zielgerichtetes Suchverhalten mit negativen Gefühlen wie Angst und Stress verbunden sein kann, sind offene, explorative Leserinnen und Leser tendenziell positiver gestimmt.
Auf gesellschaftlicher Ebene zeigt sich, dass in Ländern mit einer breiteren, vielfältigeren Neugier auch Bildung und Gleichstellung besser ausgeprägt sind. Die Freiheit, sich in verschiedene Richtungen weiterzubilden, fördert eine gerechtere Gesellschaft – und umgekehrt schafft Gleichheit die Voraussetzungen für eine offene, vielseitige Wissenssuche. Die gute Nachricht: Neugier ist nicht festgelegt. Wir können unsere Art des Fragens und Entdeckens weiterentwickeln – und so neue Perspektiven auf die Welt gewinnen. Und welcher Stil entspricht dir? Bist du eher geschäftig, ein Jäger oder doch eher ein Tänzer?
Denkanstoss zum Wochenbeginn
„Geschichte ist Ironie in Bewegung.“ – Emil Cioran (1911–1995)
ProductivityPorn-Tipp der Woche: Delegieren lernen
Du musst nicht alles selbst machen. Delegiere Aufgaben an andere, wenn es möglich ist, um Dich auf Deine Kernkompetenzen zu konzentrieren.
Aus dem Archiv: Warum Geistesblitze nicht aus dem Nichts kommen
Ich habe lange geglaubt, dass gute Ideen aus dem Nichts auftauchen. Beim Zähneputzen, auf einem Spaziergang, in der Dusche. Dieses magische „Heureka!“ – und plötzlich ist die Lösung da. Aber irgendwann merkte ich: So einfach ist es nicht. Der Geistesblitz ist nur der sichtbare Höhepunkt eines unsichtbaren Prozesses. Und je komplexer das Problem, desto weniger reicht er allein. Wer Lösungen für anspruchsvolle Fragen finden will – ob im Beruf, im Studium oder im Alltag –, muss wissen, wie dieser Denkprozess funktioniert. Dabei geholfen hat mir ein Denker, der schon vor fast hundert Jahren genau das beschrieben hat: Graham Wallas. Sein Modell der kreativen Problemlösung hat mich beeindruckt.
Vielen Dank, dass Du Dir die Zeit genommen hast, diesen Newsletter zu lesen. Ich hoffe, die Inhalte konnten Dich inspirieren und Dir wertvolle Impulse für Dein (digitales) Leben geben. Bleib neugierig und hinterfrage, was Dir begegnet!
EpicMind – Weisheiten für das digitale Leben „EpicMind“ (kurz für „Epicurean Mindset“) ist mein Blog und Newsletter, der sich den Themen Lernen, Produktivität, Selbstmanagement und Technologie widmet – alles gewürzt mit einer Prise Philosophie.
Disclaimer Teile dieses Texts wurden mit Deepl Write (Korrektorat und Lektorat) überarbeitet. Für die Recherche in den erwähnten Werken/Quellen und in meinen Notizen wurde NotebookLM von Google verwendet. Das Artikel-Bild wurde mit ChatGPT erstellt und anschliessend nachbearbeitet.
Topic #Newsletter
Rolling
from An Open Letter
Today N Came over along with a few Other friends and we played Mario party, and for a little bit beforehand, we rolled around and I haven’t gone to do that for over a year now. I do miss jujitsu.
I was also thinking about how I feel like I don’t want to settle or compromise what I’m looking for in a relationship too much, and I don’t like the idea of actively dating in the sense of dropping my standards whenever it feels like the dating pool has ran out. And I kind of wanna apologize to younger me, and also the idea of potentially being married by 30, and I still think that there’s a pretty strong chance that happens, but I think it would probably be for the best if I stop actively chasing a relationship so much. Part of me wonders if I should look for casual sex or something like that, but I don’t really know if that is something for me or good. I feel like even if it’s hard to articulate, I have a mental image of the kind of person that I really get along with, and I would like to spend my life with. I honestly feel like a lot of that is just ADHD, because a lot of the traits that I’m looking for I have a lot of overly there. But I guess I’m kind of taking a little bit of a step back from the whole notion of active dating, especially with dating apps. I’ve gone through and looked at what it is readily available, and I have gone on at least one date out out of it. I’m also thankful that my issue is not getting rejected, but rather rejecting people, because as selfish as it is, I would like to believe that in a sense there isn’t something I need to change about myself to become more desirable, it’s rather a waiting game. But at the same time that means I kind of lose agency, which is scary. Part of me wonders if I need to get more attractive or more desirable with different ways and maybe that would preemptively solve the issues or somehow expand by dating pool to people that are more desirable. I guess it never hurts to improve myself.
from Unvarnished diary of a lill Japanese mouse
JOURNAL 10 août 2026
Toujours chaud, chaud et nuageux. Dernier jour de surf. On va rendre nos combinaisons et les planches. Terminé pour la mer. On a bien profité de cette semaine, on s'est fait de nouveaux copains. On promet de revenir. Ils sont désolés de nous voir partir, pour une fois qu'il y a des filles dans leur bande... Ils sont gentils, passionnés par leur truc. Ils doivent dormir avec leur planche, je crois bien.
On rentre le cœur un peu serré. On va retrouver la ville et la pluie sur la ville Reste à faire les sacs. Shampooings traitants : on en a bien besoin, l'impression d'avoir des méduses sur la tête. Ce soir on se couchera tôt pour attraper le premier bus demain matin. Il faudra faire des courses en arrivant, ya rien à manger dans la maison à part du riz !
#surf