Want to join in? Respond to our weekly writing prompts, open to everyone.
Inspector Puissance vs. The Anime Club
from Printer's Devil Publishing
The year? 2026. A cassette ejected from the VCR player. “And that was the conclusion of our epic anime series, Speed Racer.” The room erupted into applause! July stood at the front of Mr. Crane's poorly lit classroom and watched a dusting of asbestos go into Mabel's Calpico as she gazed sweatily into “Netsuzo Trap” (thanks AskJeeves), while frenshman transfer Madeline played GameBoy Color. There were some other unnamed club members too, playing marbles and jacks, as teens are wont to do. Their friend Nicole, who is here for exactly one line, raised her fat gay hand: “[CLEARING THROAT] what comes between episdodes 5 and 8?”. July replied “6 and 7”. The three of them began snickering and dabbing and juggling their hands, braying 67 67 67! July, exasperated, sat besides the mouse cage and began stoically playing cat's cradle with scarlet twine, as Mabel and Madeline went up to present.
Today we'll be talking about my favorite anime “Boku No Pico Academia: Thrice Upon A Time” said Mabel, “and I'll be presenting on Hamtaro and Naruto!” proudly exclaimed Madeline, Gaulishly.
Down the hallway, something lurched.
July got up in a huff and immediately began arguing with Madeline, the brains of the operation.
“We talked about this last time when you showed us Junjou Romantica, you NEED to select a shonen or isekai from the approved list!!!”
“Shut up. SHUT UP! I already told her it's her favorite, you don't even read anime!”
Faintly, they heard someone scream “breach breach breach” and kicked the door off it's hinges.
“THE SCHOOL RESOURCE OFFICER!” quoth they, big eyedly and bleeding from their nostrils.
“Yes! 'Tis I, Inspector Hercule Puissance!”
“What?”
“He got shot in the head last week confiscating someone's dime bag, just go with it.”
“And I heard the Junior Crime Stoppers are going to help me go on patrol!”
“I'm sorry Inspector Hercule but we're very busy. We have lots of Dragon Ball Tales to watch. My mom said if we watch all the episodes and do a group suicide we go to Dragonland and meet Vegeta”.
“Your mother is Correct, but...” just then, Inspector Puissance drew a .44 caliber magnum from his holster and shot the anime club's projector. Acrid gunsmoke filled the air as the children cheered. July sighed deeply and went off on her weekly heroic adventure with The Junior Crime Stoppers, while Mabel and Madeline nervously hid shota magazines and obnoxious candy vapes in their backpacks.
“...And maybe afterwords we can watch your favorite from before your brain got scrambled. You told me your writer friend that passed away showed it to you. It was Princess Jellyfish.” he yanked the VHS away from July, tossed it into the air and shot it – the children cheered! “And now to solve crimes!”
The cadre moved en masse down the hallway. What crimes are usually committed in a school? Just then, Inspector Puissance detected the smell of marijuana smoke. He activated his X-Ray vision and saw a skeleton smoking in the bathrooms. He breached the bathroom door, took the joint, smoked it all one hit, screamed “JUSTICE!” then pushed Nicole's fat gay ass out the window. Told you it was 1 line.
“Inspector Puissance I don't think the school resource officer is allowed to use deadly force on students for smoking in the bathroom”. “What was that July? You're taking a vacation to Prague?” “STAWP!” JUST THEN, THE POWER CUT OUT, A FLASH OF LIGHTING, FOLLOWED BY THE SOUNDS OF SOMEONE FALLING DOWN THE STAIRS! OW THUD OW CRACK OUCHIE {SPLAT}
The backup generator turned on. Inspector Puissance stood there with July and Madeline. But where oh where was Mabel? GASP, said July! “Look at that trail of blood! What could have happened?”. Inspector Puissance took out his magnifying glass and pressed his eyeball against it, bent over, and followed the trail down 50 flights of stairs, to find a mangled mess of a corpse at the bottom of the stairs. Madeline ran to the pile of organs and bones, ugly crying. “MABEL? DEAD? NOOOO...!!!”
Worriedly, July approached Inspector Hercule; “Crime is afoot.” “Don't mention feet this early into the story he'll get sidetracked.” “What?” “Nothing, go back to the root menu so we can discuss the case. Hey real quick, can you do a vaguely Asian accent?” “I'm not going to do that detective”. The inspector glanced gallantly at the pile of gore and intestines that Madeline was rolling around in, making out with her friend's severed head as the tongue flopped around limply. “So are we thinking foul play here?” July pressed her fingers into her nose bridge and winced, as though attempting to mitigate a migraine.
“July...did you commit this murder?”
“No. No I did not commit the murder, Inspector.”
Ambiently, six piano notes played to indicate that she was telling the truth. They were both confused and looked to try to see where it had come from, when they were interrupted by maniacal cackling.
“Wrong again, Fash! Twas I, Madeline The Merciless! This was all an elaborate ploy to subvert your yankee pig american way of life! I was sent by the Emperor of Japan to sew discord with the violent imagery and foreign plotlines of anime! Every doujin is another plane in Pearl Harbor! AHAHAHA!” The Inspector unsheathed his saber – “Have at thee, Knave!” She gulped. “Hey look over there!” and after about 30 seconds they both turned to look back. [UNISON] “Hey where'd she go?”
Epilogue: Julie watched Outlaw Star with The Anime Club undisturbed the next week. The End!
Conquering the Barbarian Altanis: Session 188
 Attronarch's Athenaeum
Attronarch's Athenaeum
Adventurers
| Character | Race | Class | Description |
|---|---|---|---|
| Gerda | Human | Magic-user level 1 | Seeks to travel all over the Wilderlands to gain experience. |
| Kho Rimbo | Human | Magic-user level 3 | A knife throwing wizard extraordinaire. Covered in ritual knife scars. Cuts himself whilst casting. Prone to being sarcastic. |
| Minako Konishi | Human | Monk level 3 | Pretty Karakan with grace of a panther and shrewdness of a fox. Silk sash holds here loose trousers in place, while loose jacket rounds up her exotic look. |
| Remus | Hobbit | Thief level 1 | Sketchy hobbit looking for better loot. |
Thawmist 16th, Airday
Minako received word from Ambros, whom had been visited at Old Crus's tower by Agathon the Wiry, that a man supposedly following a treasure map hadn't returned. He left couple of weeks ago, and Agathon promised to take care of his family. Aging constable, now promoted to the Captain of the Guard by the baron, visited the exiled cleric seeking help. “Could you ask you adventuring friends to take a look? I cannot pay, but if his map was true, you get to keep whatever you find...”
And so Minako assembled a rag-team of Kho-Rimbo wearing an iron-cage over his head, and two new recruits, namely Gerda the Medium, and Remus the Apprentice. They set out at the same time as the other, larger and better armed adventuring party set out for the tumulus north-west. But Minako and her crew travelled south-east, up the hills.
They reached the described area some time around noon. It took them until nightfall to find the described caves—four entrances in total. They retreated and camped in the wilderness. Remus spent some time carefully taking off Kho-Rimbo's bridle. The cocky theurgist was humbler and quieter than usual. Sore jaw and inflamed and swollen tongue might have contributed.
Thawmist 17th, Waterday
Adventurers carefully approached the cave slits facing south. Two were to the left, and two were to the right, separated by some two hundred feet of rock. Part of the information they had is that they right place has a tunnel going from one side of the hill to the other.
They opted to approach the east side. Northern slit was twenty feet wide and nearly thirty feet tall. Limestone tunnel beyond it stretched for sixty feet before bending eastwards. Cave mouth to their left was narrower and lower, but still open. It led to a spacious cave.
A carved boulder rested on the south side of the cave. Broken and rusted pickax was next to it. Twenty feet wide tunnel to the north stretched beyond the torchlight. Shoddy and saggy net-trap was visible. Frayed ropes held it in place. Remus scaled the cave wall and severed them.
Narrower tunnel to the west led downwards, into yet another cave. Since the slope was quite steep, and adventurers were unsure if they would be able to crawl back up, they decided to follow the northern tunnel.
This led the on a long trek downwards, into wet and jagged cave with fractured floor and tiered drops. Rank smell permeated the air. The source was a large pool of murky, stagnant water. Gerda, well educated and crafty, tied a rock to her rope and measured the depth of water. Less than three feet deep.
Adventurers waded in. The drops continued, but not as dramatic as before. Soon the humans were hip-deep, while the hobbit's nipples were at risk of getting soaked.
And then Remus vanished, jerked violently underneath the water surface. He felt an iron grip around his ankle. The hobbit thrashed about. Gerda ran for the high ground which she had felt just moments before the chaos. Kho-Rimbo ran for the closest cave column and attempted to scale it. Minako observed water for an opportunity to strike.
Remus, disoriented and drowning, pulled his dagger and slashed wildly. Alas, he hit nothing. At least he managed to take few gulps of previous air. Minako struck and hit something. Kho-Rimbo abandoned his mountaineering ambitions and rushed towards Remus and attempted to pull him upwards. The hobbit pushed against the rocky bottom, and set himself loose of whatever was holding him.
All four adventurers ran north, towards Gerda whom had found a way up, and potentially out.
Indeed, they scaled up and up, until they reached a massive cave buzzing with activity—hundreds, if not thousands, of cockroaches, spiders, centipedes, and other vermin crawling all over the place. A strong, acrid smell dominated the area.
There were two tunnels to their left and one tunnel to their right. Cave itself stretched further north-east. Although wide and long, ceiling was relatively low, at perhaps fifteen feet. Many thick stalactites stuck out.
The party moved into the vermin swarm, navigating the ground. There was no way around them, only through. Gerda swung her torch from side to side, attempting to scare as much of critters as possible. It did not work. Now they were deep into their nest, surrounded by thousands and thousands of them.
“Look.”
A skeleton dressed in plate mail rested on some sort of hump. Centipedes and spiders crawled all over. And yet, a glorious, shiny battle axe reflected back the lamplight.
Minako prodded the skeleton with her spear.
What a horrible mistake that was.
Vermin, now roused and aggravated, formed three humongous swarms. Remus and Minako were not particularly worried about that. Kho Rimbo fled the cave. Gerda hesitated, but decided to remain and help her new-met friends
Alas, what a horrible mistake that was.
Remus made an improvise lasso out of his rope. Then he threw it over the skeleton. Success!
Hundreds of centipedes, roaches, and spiders crawled all over Minako. Dozens and dozens of tiny bites tore into her flesh. Same fate befell Remus and Gerda.
The trio now ran, fleeing back into the tunnel, and jumping into the pool or rank water.
But Gerda, poor Gerda, was overwhelmed by the centipede swarm; she fell, she fell into it. And multiple swarms crawled over her, and then there was nothing but void, for in this hour of great tragedy there was moment of mercy in her as she passed out from intense shock and venom pumped into her system.
Remus emerged from the water, all red and full of blisters from insect bites. He swatted away few remaining critters. Minako did the same. Then the hobbit pulled on his rope.
“Bah!”
Skeleton completely fell apart, and the only thing he managed to drag was breastplate.
They returned to the mouth of acrid cave, but abandoned that idea after seeing very active vermin roaming about.
Thus they returned the same way the came in—down the tunnel, through the pool, up the tunnel, and then east.
“How about we at least check that north tunnel?”
And so they followed this different, hereto unexplored route.
This was a spacious tunnel, of varying width as they progressed deeper and deeper. They eventually reached a point where the tunnel widened into a cave and split off in three more directions—north, north-west and south-west.
The whole chamber reeked of manure. There were four decayed wooden crates in a natural alcove by the north-west tunnel. They contained worthless, moth-eaten and mildewy bolts of cloth.
Adventurers cautiously moved down the south-west tunnel. This lead them to another cave. Another natural alcove was to their left. A large mahogany coffer was visible at the far end of the alcove.
Minako approached it boldly.
Without any warning stone above the coffer formed mouth and began yelling loudly:
“TURNU REEN, TURNU REEN, VI NAZGUTIGILOJ! Ĉi tio ne estas via trezorejo, ne via trogo, ne via necesejoŝtono! Mi estas la Gardanto de la Juglando, la Gardanto de la Kudzuo, la Gardostaranto de la Splito! Ĉi tiu kofro enhavas nenian oron – nur la akumulitajn ternojn de mil travintrantaj meloj!”
It thundered all through the cave. Within seconds barking, yelping, and howling could be heard from the south.
Kho Rimbo wept inside, unsure if he should fled now or immediately. Remus had big eyes, his thieving instincts were going ringing. Minako cared not for the noise. She grabbed the lid and jerked it up, ripping it off.
The insides of the coffer were lined with some plushy material. A folded, magnificent crimson cloak filled the volume. Monk grabbed it and pulled it up, sending gems and other valuables wrapped inside it tumble all over the coffer.
Kho Rimbo found courage and rushed up to the chest to pick up as much of it as he could. He ignored the iron hand adorned with violet garnets and kris dagger. Remus was happy to pick everything up.
The trio emptied the coffer, and fled the cave. Nonsensical yelling did not abate with them leaving.
They ran into the wilderness, and found a safe space to camp. Remus mounted brank's bridle on Kho Rimbo so he could return to Ironburg and avoid fate worse than that one. They slept well. Or, at least the monk and thief did.
Trio returned to Ironburg on Thawmist 18th, Earthday, impressing other adventurers with their haul: a left hand made of iron and decorated with six violet garnets, three candlesticks made of gold with decorative moonstones, a magnificent crimson, stitched cloth coat, one deep blue spinel, one tourmaline, three smoky quartzs, and a magical kris dagger.
Discuss at Dragonsfoot forum.
#Wilderlands #SessionReport
Pixie
from Tuesdays in Autumn
I finished reading Pixie by Jill Dawson on Sunday. The book’s eye-catching cover first snagged my attention from a bookshop shelf back in May. It’s an historical novel based on the life of the artist, illustrator & writer Pamela Colman Smith, best remembered for designing the famous Rider-Waite tarot card deck. It follows Smith from Jamaica (which she leaves following the death of her mother), via Brooklyn, to London, where, at length, she finds a precarious foothold in the city’s theatrical and bohemian circles. According to the novel, it was one of Smith’s first and most notable theatrical friends — the actress Dame Ellen Terry — who bestowed the nickname Pixie on her.
For me this was a book that had something of the ‘biopic’ about it: a series of vignettes from the subject’s rise to modest fame, with cameo appearances from all the notable names she encountered along the way. While not terribly deep or daring, it’s an enjoyable story of an unconventional character in an interesting milieu. While Smith was undoubtedly ahead of her time in some respects, I did I wonder now & then if Dawson might have been projecting a little too much of the present into her Edwardian setting. And the Rider-Waite tarot commission is presented as a culmination of Smith’s work, when it could just as easily have been just another job for her (albeit a substantial one). It would have been interesting, moreover, to read something about the artist’s subsequent conversion to Catholicism & her later support for women’s suffrage. Then again, further extending the story may have bent the narrative too awkwardly out of shape. Dawson did succeed, I think, in making something coherent and engaging out of the patchily documented facts of Smith’s biography.
A recent stationery acquisition: a quantity of old sealing wax (Fig. 33), namely John Heath’s Bank of England sealing wax (Fig. 34). I own a couple of seals but would like to find some better ones before I use this stuff in earnest. And I’ll need to practice melting and dripping the wax, after making a some ham-fisted initial attempts.
My collection of vocal jazz/pop recordings of the ‘50s and ‘60s has been augmented with the recent purchase of Ernestine Anderson’s 1960 album My Kinda Swing. My copy is a budget re-issue from ‘64 on the Wing record label – a subsidiary of Mercury Records – which omits two of the twelve tracks included on the original U.S. release. On the rear of its sleeve are a variety of other re-issue releases on Wing including the likes of Muggsy Spanier and his Dixie Land Band; Dick Contino’s An Accordion in Paris; and Music for Polka Lovers by Lawrence Welk.
My Kinda Swing the fourth of five albums Anderson made in rapid succession for Mercury. Later in the ‘60s her recording career stalled as fashions changed, only to blossom anew from the late ‘70s onwards. I’d hitherto only heard Anderson via YouTube, so it’s a delight to finally listen to her on well-recorded, well-pressed vinyl, accompanied by such expert musicians as Clark Terry, Hank Jones, Yusef Lateef, and Kenny Burrell. Among the tracks I particularly enjoyed at first hearing was her brief but beautifully languid take on ‘Moonlight in Vermont’.
We now show alt text in the fediverse! Now alt text from photos in your blog posts gets sent out over ActivityPub, so your images are more accessible to your readers and followers there.
Alt text (meaning alternative text) lets you add a description of any images you include in your posts. This is especially helpful to readers who are blind or have low vision, and use screen readers to consume your posts — instead of an empty space where your image is, the screen reader can read aloud the description you provide, giving them the full context of everything you’re sharing.
In our Plain Text editor, you can use standard Markdown to add alt text in the brackets before your image URL:
In our Rich Text editor, you can use the top menu option: Insert → Image to find a Description (alt text) field, where you can describe the image:

Alt text on Write.as has been here since day one. But especially with it carrying over to the fediverse now, we’d highly encourage writers to make an effort to include it more often in their posts!
#updates #fediverse #altText #accessibility
Only God Forgives (2013)
 The Third Alternative
The Third Alternative{kind=link}
{kind=link}
The tension in this movie is what really stays with you even after it ends.
Only God Forgives (2013) will remind many viewers of Drive (2011), and some of Valhalla Rising (2009). All three are directed by Nicolas Winding Refn and you can definitely see his signature style in all these films. I personally really like his work, but reviews are mixed for this particular film. This is no surprise because the film is not the typical Hollywood blockbuster, so many people are likely to watch it with different expectations.
Fans of movies made by Gaspar Noé will appreciate this movie. in fact, Noé visited the film set and he's being thanked in the credits. Nicolas Winding Refn was clearly inspired by Noé's work. In addition, he dedicated the film to Alejandro Jodorowsky, whose work has always beeb ahead of his time and deeper in meaning than many his fellow directors, writers and producers. The point of this whole movie trivia bit is to show the kind of movie this is, to give it a bit of lineage if I can call it that. It's not your typical date night movie by a long shot.
Out of the three, Only God Forgives seems to get the worst reputation. However, I really liked this movie and I believe it has a meditative quality, not in the sense that it relaxes you, but in the sense that you can watch it more than once and each time you can try to see deeper into the details. There are a few elements that stand out when I watch this movie: the unknown history of the characters, the silence, and the tension.
Who are These People?
The movie begins with a murder and we realize quickly that Ryan Gosling's character, Julian, and his brother Billy are criminals, using a Thai boxing club as a front while their real business is illegal. We never get too much detail of the real business other than it has to do with drug smuggling. We get the sense that Julian is an unwilling criminal, that he does not really love the life of crime. There's a sense of reluctance to what he does.
On the other side of the rink we have the local police force and Chang. I don't want to call Chang the “hero” of the film because his methods are questionable, but he's the closest thing we have to one. His aim is to restore order, and he's successful. All this sounds very generic, and as you can see there is not too much detail given. The viewer has to use the power of imagination to fill in the gaps or infer meaning. For example, Chang does not wear a uniform, and yet the other officers respect him implicitly. Is he retired? Is he not really a police officer? How come he carries a sword? He's a frightening figure to all that cross him and the sense of unknown and mystery surrounding Chang makes him even more impressive. Consequently, we get this tremendous contrast between the imposing figure of Chang who calmly restores order without mercy, and Julian, who is not a very good criminal and who can only evoke pity in the viewer.
Silent but Deadly
There isn't much dialogue in Only God Forgives. That's why we learn little about the back story or the characters aside from what we witness on screen through their actions. The silence is especially effective juxtaposed with the musical sequences. While Chang does not speak much, he does sing! There are two scenes where he is singing in a restaurant to an enthralled audience. This gives Chang a very human trait and it contrasts greatly with his violent methods. It's so interesting seeing this mysterious agent dish out justice with his sword one moment, and singing a ballad the next.
Julian is pretty quiet too, but in his case I took the silence to signify more of an inability to assert himself or to make a stand. He seems to patiently accept what others tell him and when he does reach his limit, he takes it out on the wrong people. And yet, I can't help but feel a little bad for him. When it's time for specific decisions, he shows mercy, twice, in spite of his criminal duties.
Overall, the silence allows the viewers to take in the beautiful visual style of the movie. Neon lights and the backdrop of Bangkok, interesting angles and scenes, intense close ups that let you sense what the characters are thinking and feeling. You just have to experience the movie rather than simply watch it to see what happens at the end.
I Can Feel it Coming in the Air Tonight
The tension in this movie is what really stays with you even after it ends. The tension is tangible, partly due to the minimal dialogue, and partly due to the foreshadowing that keeps popping up in various scenes. The combination creates a sense of foreboding. You just feel something bad is about to happen. Everyone on the screen is on the edge, especially the criminals, but less so Chang. In fact, Chang's calm sense of control is like an anchor amidst all the tension. You just know that nothing can stop Chang: he is a force of nature; not a wild tornado, but more of a slow steady snowfall that will eventually bury everyone. All they can do is pray for mercy, but as the movie title tells us, only God forgives.
Thank you for reading! #review
Bookmoms
from The Lantern Room
Children are made readers on the laps of their parents.
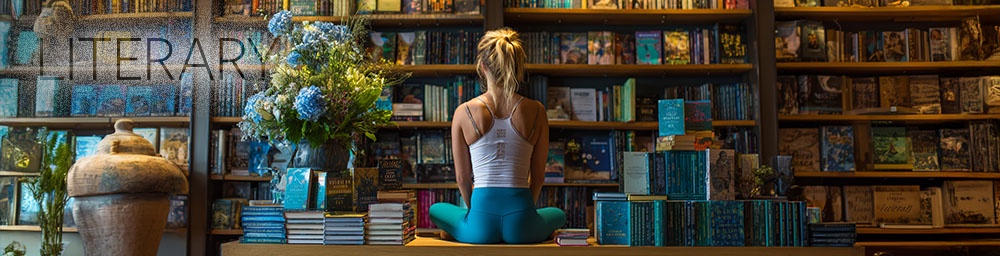
She reminds me of someone else. Excellent posture, moving with the grace of a dancer and clearly very at home among the stacks of books. A fiction-reader based on her current orbit.
I don’t intend to luridly stare, but her ensemble is hard to ignore: teal toenails (matching fingers) and white flip-flops, royal blue yoga pants (painted on), and a draping T-shirt that hangs gently from her chest—just short enough to act like a curtain over her torso without revealing skin. Modestly immodest.
From a distance, I thought her much older. Up close, she looks barely 30, if that. She speaks gently to a 12-year-old girl curled up in the easy chair next to me, bottled up with a book. I want to glance at the title, but feel like I’ve already used up my karmic grace on recording mom.
Young mothers still have the energy to be moms and retain a semblance of their own identity. She’s trying—perhaps too hard—to stay beautiful, put-together. Many simply throw in the towel. (I think of the full-bodied women staffing the shelves, the checkout, the coffee counter—tired faces, hair tied back with function, not flair.)
The young mother continues to drift through the aisles, flipping through displays and kiosk stands. Her hair is pulled into a bun, held loosely with just the right number of deliberate stray strands. No doubt carefully assembled.
I wonder what instilled a love of books in her little girl. Maybe it was Dad. Or a great teacher. Or maybe Mom curled up beside her when she was small, and now she still seeks that same comfort and escape between the book boards.
No child has ever gone wrong seeking safety in stories. And God bless the mothers who made their love felt through books.
#reflection #essay #memoir #journal #osxs #100daystooffset #writing #books
2025-07-29 11:45:00
——————————————————
It's been a while
from Chris King
It really has been. A very long while in fact, since I last sat down and wrote.
Not writing in general – I'm doing more of that than ever, though increasingly for non-human recipients – but writing an article, under my own name, sharing some personal thoughts on things I find interesting.
There's a reason for the absence: for the past eight years I've been busy building GRID, the data platform used by game developers and tournament organisers across the industry to power the official data layer for their esports. Back in 2018 esports data was a fragmented, fledgling space and GRID was just a handful of passionate people huddled in a Berlin coworking space, hellbent on changing that.
Today, GRID is over 100 people strong, and partners with names such as Riot Games, ESL FACEIT Group and Ubisoft, providing platform technology to enable a data layer used by competitors, fans, analysts and businesses across the globe. It's been an incredible journey.
So, a (re)introduction. Hi – I'm Chris, co-founder of GRID Esports, where I've spent the past eight years building and leading our product and engineering efforts as CTO.
These days, much of my energy goes into where the technology takes us next.
I think of myself as a product-focussed technologist. I love truly useful tech – not just the kind that does wildly complex things in elegant ways (though that too), but technology with a real purpose. The kind that becomes part of the foundations – that others build on, that outlasts its makers' attention, and that leaves its corner of the world working better than before.
It's this tenet – the thing that gets me up in the morning – that has me wanting to make time to write down a few thoughts more regularly.
You can probably guess what comes next. Yes: the world is in the early stages of a technology shift bigger than any that came before it. Those of us in software are seeing it first-hand, and earliest. AI systems this capable and with such general application won't leave any part of society untouched.
But for all the road that lies behind us, most of it is still ahead. And I believe the discipline of building things that are truly useful and built to enable sustainability, will decide whether AI gets woven into society well, or badly.
So that's what I'll be writing about: engineering useful, sustainable products in the age of AI, and what it takes to lead an organisation through changes this impactful. With a strong likelihood of some esports and data content mixed in, but surely that comes as a surprise to no-one?
Until next time,
Chris
from Blog of Sand
Anthropogenic Climate Change Feedback Loops
There has been a lot of attention paid to climate feedback loops that occur in nature. Permafrost thaws, releasing trapped methane (a potent greenhouse gas), raising temperatures, leading to more thawing, and more methane release, and so on. The same is true for polar ice caps melting and changing global albedo, increased water vapor in the atmosphere (water vapor is actually a very potent greenhouse gas) and forest fires. However, I haven't seen as much discussion as how it may effect human behavior.
Here is one that worries me. Many nations in both the developing and developed world have pretty low utilization rates of air conditioning. However, climate change is causing dangerous heatwaves, leading people to reconsider. Suddenly, Europeans might be swapping out having the windows open for a natural breeze with electric powered air conditioning. India, as it modernizes and access to air conditioning spreads, could see tremendous proliferation. Etc etc. More air conditioning means more electricity demand. While some of this may come from renewables, rapid spikes in demand generally require some fossil fuel deployment to address. This means more greenhouse emissions, which means more warming, which means more air conditioning demand. You get the idea.
These human behavior based feedback loops may individually be relatively small, but on the aggregate with natural feedback loops could be a major issue. It's too hot to walk anywhere so people drive. People fly and drive to cooler areas in the summer, traveling more which increases emissions. Drought necessitates desalination which requires a lot of power demand.
A big one that I don't think is talked about enough is climate refugee crises. If large swaths of the world become relatively uninhabitable either due to extreme heat, drought, flooding, etc, people are going to want to move. And with xenophobia and scarcity mentality, countries frequently aren't exactly... friendly to refugees. This leads to polarization, militarization and frequently the election of more nationalist/authoritarian leaders. This correlates with heavier fossil fuel usage and less environmental steweardship. Just another thing to consider.
Of course, there are negative feedback loops. More carbon means higher plant growth. Climate disasters hurt economic output and dampen emissions. But overall, I think the vibe is that the positive feedback loops are much stronger. I'm not sure what the tipping point is, but more and more I think a rough ride in the 2040s-2100s is mathematically baked in.
hello, log
from  blog//x2600.cc
blog//x2600.cc
10:28, cereal with coffee creamer. Coffee
I am helping with bukmark.club by answering the call from it's maintainer to find dead links in the directory. I got through A-J, will do more soon. I emailed the maintainer with said links. Good service.
Whole
from The Lantern Room

We become what we love.
I love sunshine. I wake up every morning and the first thing I do is acknowledge how much light is in the room. It will be funny when I move and can no longer tell the time, because here, I can tell within 15 minute intervals what time of day it is.
A room filled with morning light is among the greatest of my pleasures. If it were up to me, every room in the house would have big windows into which light would spill all day long. Great rectangles serving as sundials.
I was reading this morning about loving Jesus, thinking like him.
Since Christ suffered in the flesh, you too arm yourselves with the same mental disposition. — 1 Pet. 4:1
“You must love Jehovah your God with your whole heart and with your whole soul and with your whole strength and with your whole mind.” — Luke 10:27
Jesus acknowledged this as the most important command in the Mosaic Law. Notice that our love for Jehovah involves our heart, which includes our desires, feelings, and emotions. It also involves our whole-souled devotion and our strength—including our energy.
However, loving Jehovah also involves our mind, which includes the way we think about matters. Of course, we can never fully understand all of Jehovah’s thinking. But we can better understand God’s thinking by studying “the mind of Christ” because Jesus perfectly reflects the thinking of his Father. — 1 Cor. 2:16
I like the commentary because it defines our whole being: desires, feelings, emotions, our energy, mind, thought.
These are reasonably put into two categories:
HEART 💙: desire emotion feeling
MIND 🧠: logic thought energy (this one arguably could go either, but we need symmetry, reader!
I was always of the mind that the second category was fully controllable. That we just switch on thought-control and we can Vulcan our way out of anything.
But I discovered last year that our biology can override our ability to think. I was waking up every night at 3 am in tears. I would curl up on the floor and wedge myself under the bed because it was the only place I felt safe. For three hours I would pray, and cry and listen to music or meditative spoken word recordings to try to engage my mind. it was STUCK on feedback loops of everything wrong in my life. Bad decisions, family strife, childhood trauma, work, death, overload, loss—you name it, i was anxiety-maxing about it.
This went on starting in April through August when I finally saw a doctor. And with the right drugs, the chemistry that was starting the cascade was stalled.
The heart, however. Even the Bible says it's treacherous. It's this wild thing that can burn worlds or save a soul with nothing more than words.
and sometimes, it's the heart that reigns in our brains.
This is why I love Nick Seluk's' The Awkward Yeti
https://www.theawkwardyeti.com/
Few thinkers capture the dynamic quite as well as his heart/mind characters. Funny, I rarely see the actual yeti in this strip.
We are most powerful when our minds and hearts are unified in pursuit of goodness. How goodness is defined changes based on whom you ask.
And a wise person will always ask the Maker what is good. And sometimes we'll get a definite answer, others we'll get a 'well, it depends'.
It's in the 'it depends' zone where we get to be whatever we want. Giving a gift? What should you give? Well, it depends. Don't give a diabetic a basket of sugar, but beyond that... could be something you like, something they like. Could be just note or letter.
Whatever good your hand finds to do, do.
Sometimes the best 'good' we can do, is nothing at all.
If we truly love God and try to follow the example of his son, we'll be just fine. We won't get it right all the time. IN fact we'll get it wrong a lot. Sometimes, most of the time. From time to time, all of the time.
The important part of the equation is that we never give up, ever stop trying. That's what 1 Peter 4:1 is really saying. 'Arm yourselves'. Master that tool and it's a force multiplier. But it isn't a magic talisman. No soldier is infallible nor is he un-injure-able.
But, to be armed is to be prepared for the war of life. And it means that even though we lose a battle here and there, we can be victorious in the war of our lives.
OH! The sun has climbed beyond shadow-making on this box-shaped hole to the world, that means it's time to ambulate. I think I smell breakfast!
And then—your Keeper has to get to the salt-mines!

Last Thoughts:
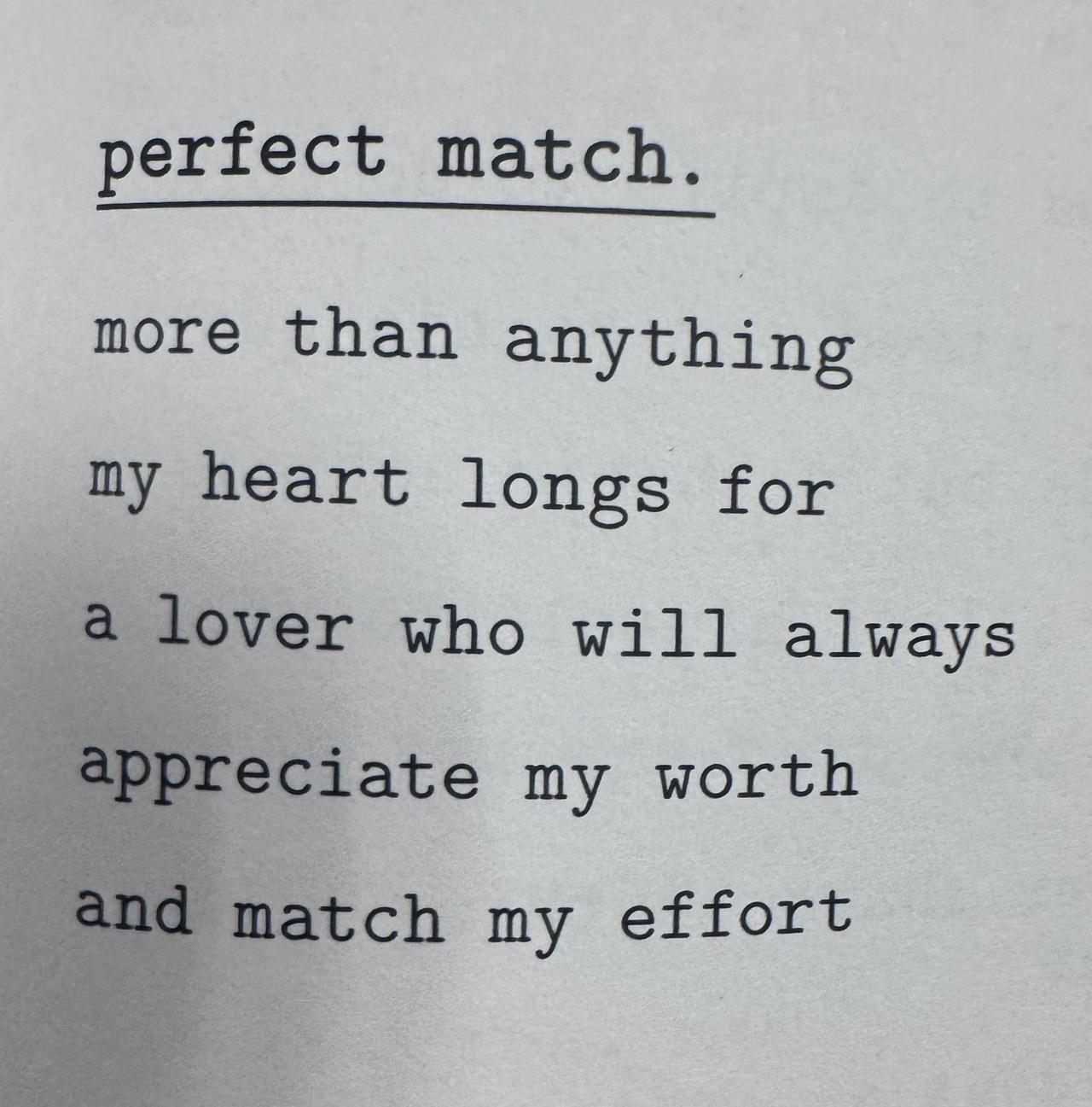
I saw this and realize the writer intended this to be 'Lover' in a romantic sense. But framed through the lens of the discussion above, what greater lover can we have than God? Only through the Creator are we truly appreciated and not only matched but exceeded.
Perfect Match, indeed!
💙💜💙💜💙💜💙💜💙💜💙💜
Isa 42:17 “I will lead the blind in a way that they do not know And cause them to tread on unfamiliar paths. I will turn the darkness before them into light And turn the rugged terrain into level land. This is what I will do for them, and I will not abandon them.”
We did not get any snow today.
from  Its_still_today
Its_still_today
This might seem largely inconsequential, but today is yet another day that I have not seen snow. Granted, snow is not one of those universal experiences and I live in a place where snow is a statistical improbability. But between the forecast of snowfall over the past week and promising early reports from yesterday gave me hope that today would be the day. It was only bolstered by being woken by reports and video of snowfall not even an hour away from me, and there was even a minute where the rain looked unlike anything I had seen before. But alas, the skies are clearing, the mercury is rising, and once again, I have been denied that simple pleasure of experiencing snow.
It started back in university a short lifetime ago. There are photos of the campus grounds being completely white for the period of a winter afternoon. It’s also an afternoon where I sat for a four-hour exam. I don’t even remember the content of said exam, only that I had missed snow because of it. And it was a basement venue so I didn’t even see it.
I’d arrived at places a day after all the snow thawed out. I’ve flown out of New York hours before a blizzard. I had a flight delayed because of unexpected snowfall at the destination, and it was all gone by the time I’d arrived hours later. I’m pretty sure that if I were to schedule a trip to Antarctica, the CO2 of the flight there would be the straw to trigger a global warming failure cascade, and we would land on the lost continent under the ice.
Knowing my luck, it may never happen. Life moves on. (Or it drives me into a conspiracy tailspin where I start trying to prove that snow isn’t real and it turns out to be the most financially lucrative thing I’ve ever done.)
There’s nothing to this at all. It is largely unremarkable in the grand scheme of things. Life doesn’t owe me snow. No grand injustice will be resolved, nor will the presence of snow improve my situation in any material way. But the way snowfall eludes me is really starting to piss me off. Today, a lot more than any other time.
It’s a matter of agency. There are times where I missed out on snow because life happened. There are times I’d made conscious decisions, partly because it would put me in a place and time where I would likely see snow.
I want to ask the universe, what do I have to do to get this one thing I want? And a little voice in my head says that there’s nothing I can do. It’s simply impossible. And it’s not just talking about the snow.
I’m not in a good place mentally. I don’t think a lot of people are. In the grand scheme of things, I’m probably luckier than most other people and have nothing to complain about. Doesn’t change the fact that it feels like there are no real options. No meaningful direction to take for… anything really. Maybe I could grasp at the last straws all around me and arrange them into the general shape of an actionable plan. Stop feeling sorry for myself, put my head down, power through, and make something that works.
But I don’t feel like it anymore.
People look at me like I’m insane when I say that.
When I say I don’t really want to do anything.
That I don’t want to work for the opportunity to do harder work that might just get me to the point of earning a respectable living again.
From where I stand, it didn’t really matter the last time I did the same. Got good grades, got into college, got the degree, the big tech corporate job, been there for the family, been the team player, been generous, been smart, been ethical, been ambitious, been honest, paid dues, showed loyalty… Everyone else I know who went that route are in the same boat.
Because it turned out that the recipe for success is the opposite. Needed to be ruthless. And avoid accountability at all costs. And exploit every relationship and gaslight people that relied on me by undermining their efforts. Live off debt, put everything on some meme stock or crypto to 1000x it overnight. And break as many things as you can so you can sell the same thing back as innovation. And talk out your ass. Say what people want to hear, because who actually cares about the facts?
So what was all that other stuff for? The people I worked for made a ton of money. I’m literally poorer today than any other point of my life. After 15 years of practically killing myself. And for the last few months, all I can think about is how it was impossible to give me anything more than I “earned.” About how I should be ashamed for even asking. About how everyone has it just as bad and I don’t have real problems.
I know that life is unfair. I know the world doesn’t owe me anything.
But is it wrong to ask for at least one thing I want to just fall out from the sky? Even if it’s just a bit of snow.
from librasun.scorpiomoon
Writing Raw
Writing raw is where the truth lives before my brain gets the chance to second-guess it.
It’s my space.
It’s the one place where my mind gets to dump all my feelings without having to be palatable, polished, or okay; I just get to be completely real. I can put it all down, and when I leave it on the page, I don't have to carry it all by myself. Anymore.
Later, I can go back, reread it, and ask myself if I still feel the same way. It’s not even about “growing”; it’s about looking back without judgment and figuring out if those thoughts came from a place of anxiety or from my secure center. I don't have to apologize for being who I was in that moment, but I do get to see if I view things differently now.
Writing raw is just so relieving. It’s like setting down a heavy backpack I didn't even realize I was carrying. It gives me the breath and the distance to think, figure things out, or just sit back and say, “Okay. I hear you. Now where do we go from here?”
from  Roscoe's Quick Notes
Roscoe's Quick Notes
Tuesday night's MLB Game in the Roscoe-verse has the Detroit Tigers playing the Cleveland Guardians with a scheduled start time of 5:40 PM CDT. As I usually do, I'll follow the game's scores and stats in real time via MLB's Gameday Service where we can also find links to the radio-call of the game provided by announcers of either team we choose.
And the adventure continues.
Eclipse
I am the sun I gaze below, looking The green sky, changing colours Eclipse today
You are the moon Hiding my face Eclipse today
Our shadow, dancing For the people below
Now you are here Now you are gone
We touch in the sky of our memories
#poems
morning coffee,.morning writing
from blog//x2600.cc
7 AM, the coffee is sipped, breakfast eaten, looking at SDF, domain propogation. The site looks good, is live, but also hits me with a MetaArray page on occasion. I'll get it sorted.
A bit of resignation
from An Open Letter
I loosened my filters on Hinge, And I started talking to a few people, nothing too serious yet. But I guess I am going to listen to the advice of a lot of people and have a “roster”. Basically, just talk to several people on dates one at a time and not getting anything else until that person resolves. I feel a little bit like a fuck boy, but I guess it is naïve to think that come across might be the one. I feel like ultimately it is putting too much pressure on it and that is ultimately detrimental. I’m at least happy I am not lying to anyone or anything like that, but I think after this month of Hinge premium ends I am going to take a break from it for a little bit.